





Post-Christmas Behavioral Change: What are the processes?
There are many definitions of psychology, but most of them share a common element that defines psychology as a science that seeks to help change. Generally, the objective pursued by a psychologist is that there is, after therapy, a variation of a certain behavior of the person or group that is defined as problematic by the client. Depending on its nature, the psychologist will try to reduce the behavior (smoking fewer cigarettes for a smoker, have fewer tantrums for a child with behavioral problems,…) or increase it (doing sports in a person with obesity, engaging in interactions with people in a social phobic,…).
However, before focusing on behavioral change, the psychologist must face an even more complex challenge: motivational change. This step must always precede the actual intervention because it is easier for those who are willing to change to change. It is important to know in which motivational state the client is in order to know change is feasible.
Prochaska and DiClemente in their model of the stages of change identified 6 stages that symbolize 6 realities that any person goes through in a process of change. This model, which was initially raised in the context of smoking, has proven to be consistent in any type of change process, both a change made by oneself and a change made with the help of a therapist.
Precontemplation: The person has not yet considered that they have a problem or need to make changes in their life. Consequently, they do not usually come to therapy on their own.
Contemplation: The person considers and rejects change but at the same time feels ambivalent. Although they are aware of the problem, the balance that includes the reasons to change and the reasons to continue the same is very balanced.
Preparation: Also called the “Determination” stage. The person is motivated towards change, which for the therapist is a window period to advise the most beneficial therapeutic resource. If the person is not able to advance to the “Action” stage, he or she will go back to the previous stage.
Action: The person is involved in actions that will lead to a change, so the goal in this phase is to change the problematic behavior.
Maintenance: Attempts are made to maintain the change achieved in the “Action” stage over time and prevent relapses.
Relapse: The person returns to the behavior that had changed or was in the process of changing. After this, the subject returns to an earlier stage; it is the therapist’s job to motivate and comfort the patient so that the regression occurs at a stage as close to action as possible.
In the illustration below, you can see the 6 stages of the model:
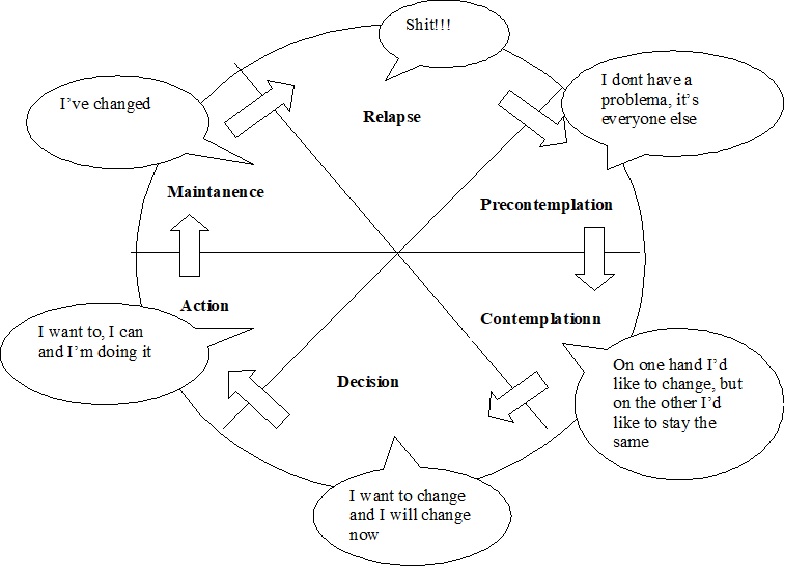
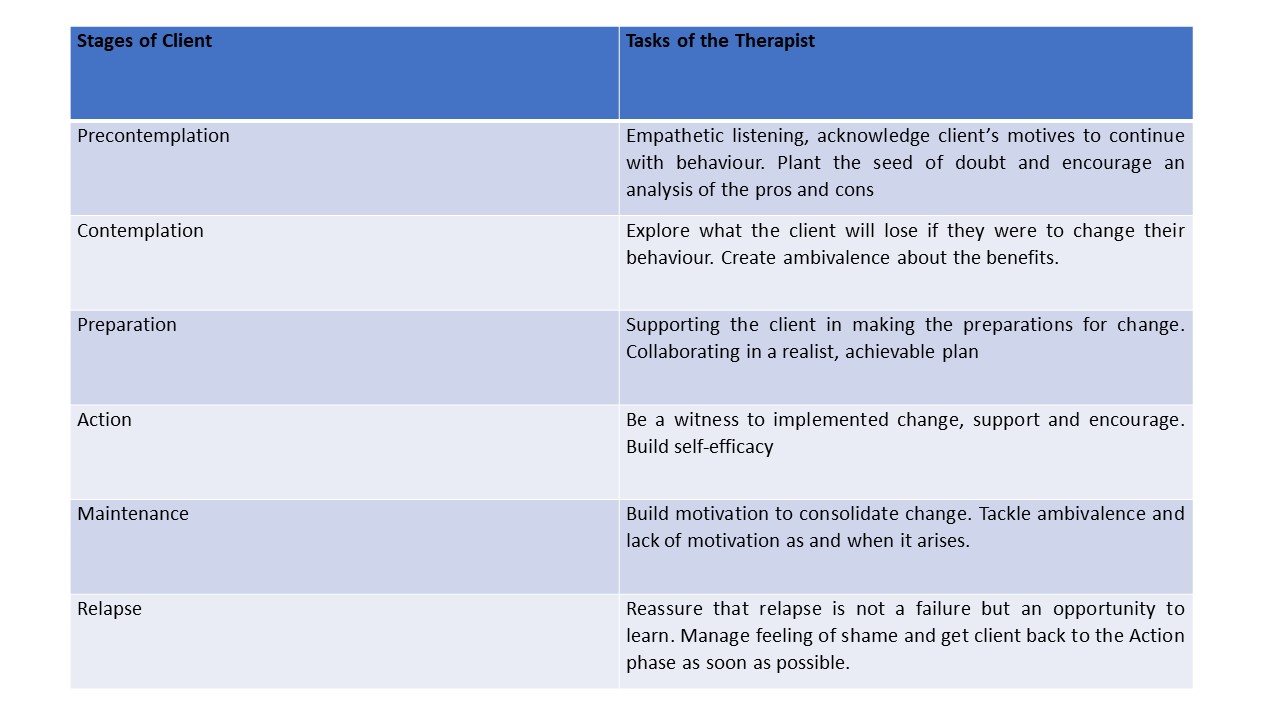
Some observations about the model should be highlighted. First of all, these stages of change are usually represented by a wheel to symbolize the fact that the person “turns” around the process several times before achieving a stable change. On the other hand, the model considers relapses as a normal event in the process of change and patients are often told that each relapse “brings one step closer to full recovery.” This is not intended to encourage relapses, but to motivate the patient to continue with their process of change. The implication that this model has in the clinical context is key since it gives an essential role to the identification of the stage in which the patient is situated, since this will determine which strategies the psychologist should use in therapy. The first stages require motivational techniques while in later phases cognitive-behavioral techniques will be applied to achieve change. The following table provides a brief summary of what psychological techniques to use at each stage:
Considering the stage of change in which a patient is situated should be a priority within the evaluation process that a clinician performs on a patient, whether it is a problem of addictive behaviors or a change in behavior. Once this has been established, techniques must be applied to move the person forward through the change process until the goal of maintenance is reached. Applying tasks that do not fit the reality of the patient will surely produce resistance in the patient that will possibly cause the abandonment of therapy. And it is that in the words of Miller and Rollnick, “therapeutic resistance appears when the therapist uses the wrong strategies for the current stage of the patient”.
If you or someone you know are experiencing difficulties in change, you can find professional help in the ESHA Spain business directory
Reference
Miller. W & Rollnick. S (2002) Motivational Interviewing: Preparing people for Change. The Guilford Press
Leave a reply
{kind=link}
Leave a reply